
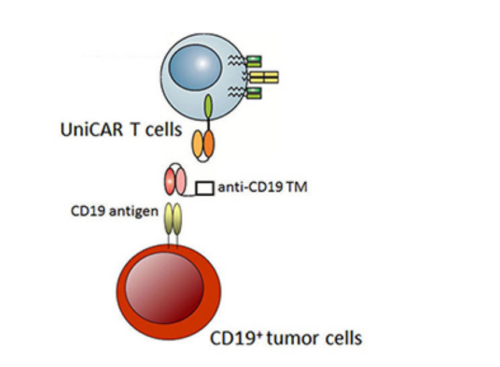
 Figure 1. The concept of UniCAR-T cells.
Figure 1. The concept of UniCAR-T cells.
In the presence of target modules (TM) against the CD19 antigen, UniCAR-T cells are cross-linked to CD19+ tumor cells, which leads to their apoptosis. In the absence of the TM, UniCAR-T cells will automatically be switched off (Bachmann, et al; Retargeting of UniCAR T cells with an in vivo synthesized target module directed against CD19
positive tumor cells. Oncotarget.2018; 9: 7487-7500.
Retrieved from https://www.oncotarget.com/article/23556/text/
used under CC BY 3.0
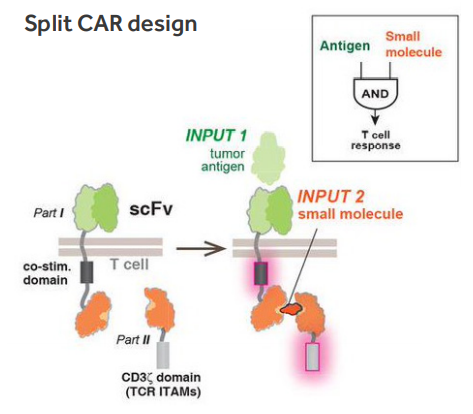 Figure. 2. Molecular strategies to control T cell activation (Wu 2015).
Figure. 2. Molecular strategies to control T cell activation (Wu 2015).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4721629/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4721629/bin/nihms751362f1.jpg
The similar method of pharmacological regulation of CAR-T cells activity is a model where administration of antibiotics like doxycycline induce expression of fully functional CAR in recipients, enabling accurate control of their activation after infusion (Sakemura 2016, Gu 2018). This apparently safe mechanism also has limitations, like the relatively slow induction and/or decreased expression of receptors. However, residual CAR expression has been observed, even in the absence of an inducer (Sakemura 2016, Gu 2018). This type of dose-dependent pharmacological regulation could allow precise control of a treatment’s duration, location and level of CAR-T cells activity, thus reducing toxicity.
Allogeneic approach – the idea for off-the-shelf product.
Although approved autologous CAR-T therapies work well without inducing graft-versus-host disease (GvHD), the time needed to prepare CAR-T cells from T cells that are isolated from patients is too long (about 2-6 weeks) and the disease may progress further before starting CAR-T treatment. In some cases, patients did not receive treatment due to the rapid disease progression (Schuster 2017, Maude 2018).
Therefore, an interesting solution seems to be the use of allogeneic T cells as an off-the-shelf product, which can be delivered to patients without manufacturing wait time. The use of allo-CAR-T cells carries the risk of developing dangerous alloreactivity, although clinical observations indicate that this is a relatively rare phenomenon. By 2018, from 132 patients with B cell malignancies treated with allo-CAR-T cells, 4% (n=5) and 3% (n=4) developed acute GvHD and chronic GvHD, respectively (Smith 2018).
To avoid GvHD, two approaches are currently being used: immunosuppression by administration of fludarabine and cyclophosphamide or alemtuzumab (anti-CD52 monoclonal antibody) prior to allo-CAR-T cells infusion (Qasim 2019) or depletion of TCR (Torikai 2012), unless the donor is a human leukocyte antigen (HLA) match. Another unfavorable situation is the reaction of the recipient lymphocytes against allo-CAR-T cells (host-versus-graft), therefore the inhibition of β2-microglobulin expression is investigated (McCreedy 2018).
A completely new approach widely studied recently is the use of gamma delta (γδ) T cells or natural killer (NK) cells as source of an off-the-shelf CAR modified cells. A natural lack of classical HLA restriction makes these cells optimal candidates for allogeneic cell therapy (Fleischer 2019).
Production time shortened – Fast CARs.
CAR-T cell manufacturing is a time-consuming process, e.g. in phase 2 clinical trials for Yescarta, it took 14 – 51 days from T cell collection to delivery of a product (https://www.fda.gov/media/108788/download). Some of the patients cannot wait that long and researchers are working on speeding up the production process. Recently, Gracell Biotechnologies received IND approval from China NMPA for its FasTCAR therapy for the treatment of relapsed or refractory adult B-ALL with the possibility of preparing autologous CAR-T cells in just two days (https://www.prnewswire.com/news-releases/gracell-biotechnologies-receives-ind-approval-from-china-nmpa-for-gc019f-a-fastcar-enabled-car-t-therapy-for-the-treatment-of-relapsed-or-refractory-adult-b-all-301209901.html) (Fig. 3).
Which of the improvements in cancer treatment using CAR-T cells described here will find wide application is difficult to predict today. Molecular biology is constantly moving forward, giving researchers tools to better understand the complex biology of cancer, as well as providing tools to design innovative cell therapies.
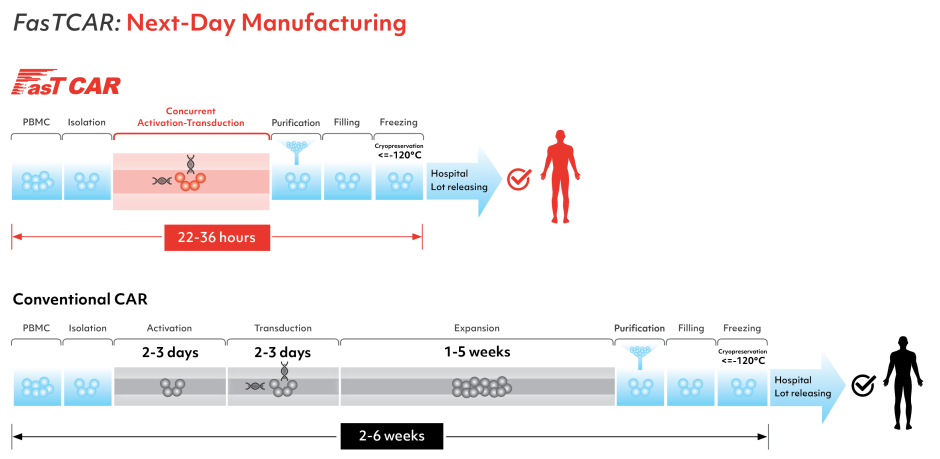
Figure 3. Comparison of the current production method of CAR-T cells with the FastCAR system.
https://www.gracellbio.com/fastcar/
https://www.gracellbio.com/img/Gracell_Workflow_FasTCAR.png)
In the next upcoming blog article, we would like to switch gears and introduce our readers to TCR-T based therapies, to which we would like to kindly invite you to read.




{kind=link}
{kind=link}