Among various treatment modalities, cell therapies have shown promising results in clinical trials, especially for the treatment of haematological neoplasms. Chimeric Antigen Receptor (CAR) T lymphocytes (CAR-T) in particular have attracted considerable attention from both academia and industry. This interest is largely justified by the FDA approval of three solutions for the treatment of leukemia and lymphoma (KYMRIAHTM 2017, YESCARTATM 2017 and TECARTUSTM 2020). Furthermore, FDA has granted fast track designation to autologous anti-BCMA CAR-T (PBCAR269A) for the treatment of relapsed or refractory multiple myeloma. To know more about CAR-T cells, CAR structures, subsequent generations or approved therapies please have a look at our previous blog article “Future perspectives for CAR-T cell therapies”.
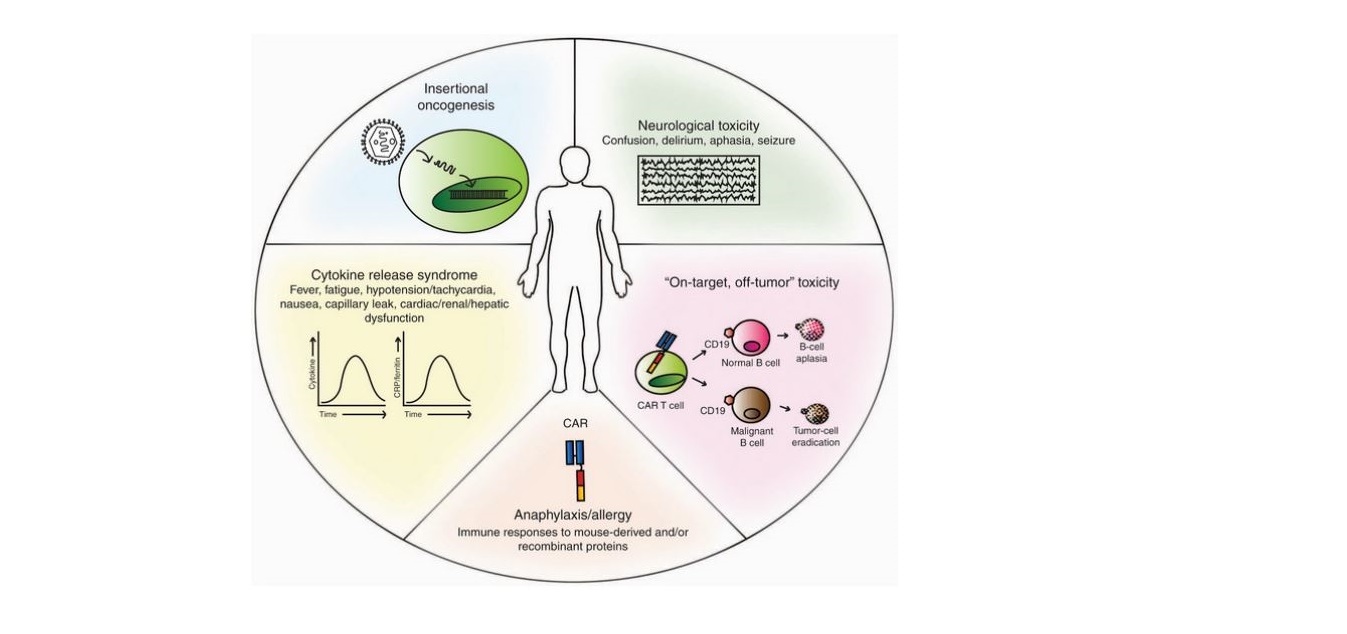
Chemotherapy and radiation kill healthy cells along with cancerous ones whereas CAR-T cells therapies are designed to target and kill cancer cells with more precision. Additionally, by the use of autologous T cells in CAR-T cells manufacturing process graft-versus-host disease (GvHD) can be avoided. Despite such a carefully thought-out and precisely prepared way of treatment, toxic effects of varying severity are observed in most patients undergoing therapy. An activation of CAR-T cells, that is necessary to kill the cancer cells is also a main cause for the toxicities like cytokine release syndrome (CRS), neurotoxicity (NTX) and B cell aplasia (low numbers or even absence of B cells) [1, 2].

Cytokine release syndrome (CRS)
The antigen recognition by CAR-T cells leads to their activation. As a result, it causes the rapid proliferation of CAR-T cells, massive cytokine production and induction of apoptosis of target cells. The release of high amounts of cytokines promotes deterioration of tumor cells, but also activates yet more white blood cells that release cytokines, which is known as CRS. Among others, interferon gamma (IFN-?), granulocyte-macrophage colony-stimulating factor (GM-CSF), interleukin (IL) 10 and IL-6 are produced. The common clinical symptoms of CRS are fever, nausea, anorexia, renal or cardiac dysfunction, tachycardia, hypotension and hepatic failure [3]. The severity of the patient’s response to the massive production of pro-inflammatory cytokines varies greatly and depends on many factors. In clinical trials, 4 grades of CRS are distinguished. The first 2 grades correspond to mild symptoms whereas the grades 3 & 4 require additional treatment because they characterize life-threatening conditions [5]. In selected clinical trials for the treatment of relapsed/refractory B-cell acute lymphoblastic leukemia with CD19 CAR-T cells, the incidence of severe CRS (grade 3 or 4) has fluctuated between 13 and 45 percent [6, 7, 8]. Mild CRS develops in most patients treated with anti-CD19 CAR-T cells and no correlation was noted between the severity of side effects and the effectiveness of treatment. In this context, it seems extremely important to appropriately determine the grade of CRS at an early stage in order to select an effective method of inhibiting this uncontrolled inflammation without affecting the anti-cancer response. Currently, in order to counteract associated side effects (grade 2 or higher), physicians use a monoclonal antibody blocking IL-6 receptor (tocilizumab) and/or systemic administration of corticosteroids (e.g. dexamethasone). The use of dexamethasone or methylprednisolone, as shown by studies, quickly and effectively inhibits CRS, but generally does not affect the anti-cancer response. Only in high doses with prolonged use (over 2 weeks) it has shown the slight reduction of effectiveness of CAR-T cells [9]. Usually, a steroid treatment begins with the administration of small doses of dexamethasone (2–5 mg/dose) and if they do not bring the expected benefits, the dose is gradually increased up to 20 mg/m2 per day. Alternatively the usage of methylprednisolone at a dosage of 10 mg/kg per day can be proposed instead. If the therapy of CRS is successful, the dose may be reduced or even discontinued [10]. Furthermore, another common practice is the administration of tocilizumab (8 mg/kg every 8 hours as needed, no more than 3 doses in a 24 hour period or a total of 4 doses are recommended (Package Insert-YESCARTATM (fda.gov)). It can be applied both as an alternative of corticosteroids or in combination with them. Tocilizumab is less effective than corticosteroids, therefore usually is used in mild CRS conditions. Furthermore, it has been reported to reduce the amount of side effects without deteriorating the effectiveness of CAR-T cells [6, 11].Neurotoxicity (NTX)
NTX manifests itself with many neurological symptoms related to the changes in the white matter of the brain tissue. These include confusion, headache, lethargy, delirium, expressive aphasia, obtundation, myoclonus and seizure. The mechanism of damage is not fully known, but it seems that the main role is played by cytokines and/or immune effector cells crossing the blood-brain barrier [3, 4]. NTX usually occurs after the onset of CRS, and often after its resolution, importantly, it can rarely present in the absence of a previous CRS [6, 7, 5]. Most NTX is mild and self-limited, the time of occurrence varies within the range from 4-10 days after the infusion of CAR-T cells. The severity, kinetics and clinical symptoms of NTX may differ between those receiving different CAR-T cell products and now, with proper treatment in a majority of cases has been reversible [9, 5]. Detailed analysis of the cerebral spinal fluid from NTX patients has shown elevated levels of cytokines including interferon-?, IL-6, IL-8, IL-10, monocyte chemoattractant protein-1 (MCP-1/CCL2) and granzyme B [12, 13]. The median duration of neurological symptoms ranges from 5-14 days [7, 12, 13] and as it mostly takes place after the occurence of CRS, therefore usually patients are already hospitalized. Treatment methods of NTX vary from center to center and are based on clinical observations and depend on the symptoms severity. Neurotoxicity grading assessment is based on 4 grades as in case of CRS. Patients with grade 1 are usually admitted to the hospital for monitoring but drugs are often not administered. If symptoms worsen to grade 2, corticosteroids, like dexamethasone, that have good central nervous system (CNS) penetration are usually considered and are often selected as a first-line therapeutics for NTX treatment. With the higher severity of NTX symptoms (grade 3 and 4), the dose of corticosteroids is gradually increased (10 mg every 6 hours) or methylprednisolone is introduced instead/- concurrently (1 gram every 24 hours) and patients also require additional tests e.g. continuous EEG monitoring, head imaging to assess for abnormalities, such as edema or hemorrhage [5, 10]. In the absence of concomitant CRS the use of tocilizumab is generally not recommended in NTX treatment as it does not cross the blood-brain barrier and may paradoxically increase the concentration of IL-6 in the CNS [12, 14, 15].